

Back pain is common and often linked to muscle strain, posture problems, or temporary disc irritation. Most cases settle with time, movement, and simple care. A complex spine case is different. When pain persists, involves nerve symptoms, or reflects deeper structural problems, doctors must investigate further to identify the true cause and guide appropriate treatment.
Consulting Dr Purnajyoti Banerjee, an experienced spinal surgeon in London, helps determine whether back pain is routine or complex. This guide explains what makes complex spine cases different.
The Quick Difference: “Mechanical” Back Pain vs a “Complex Spine Case”
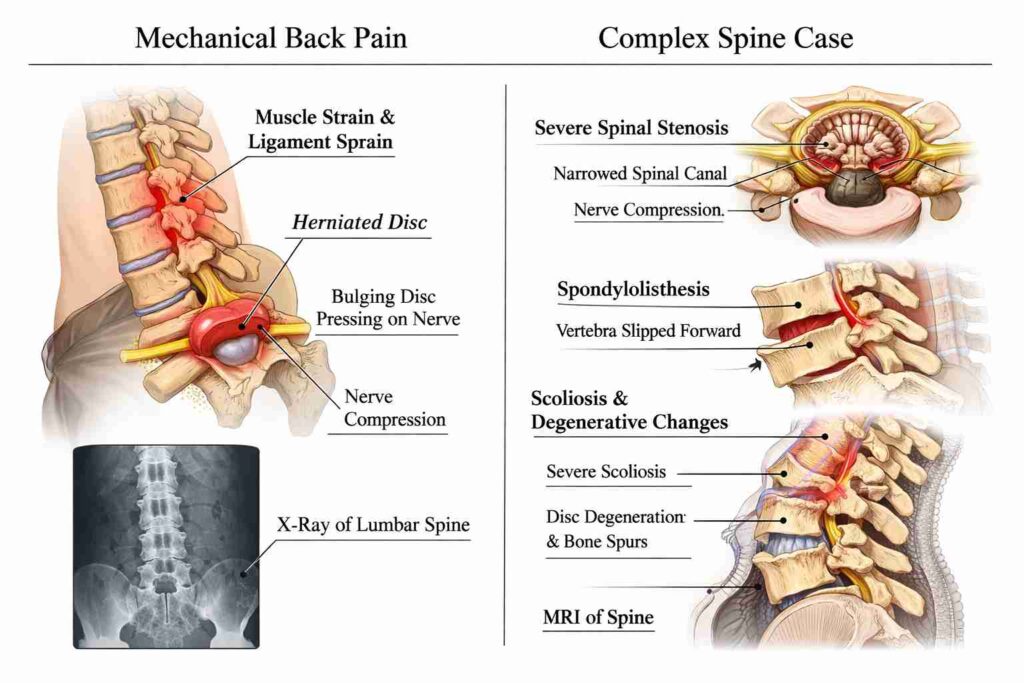
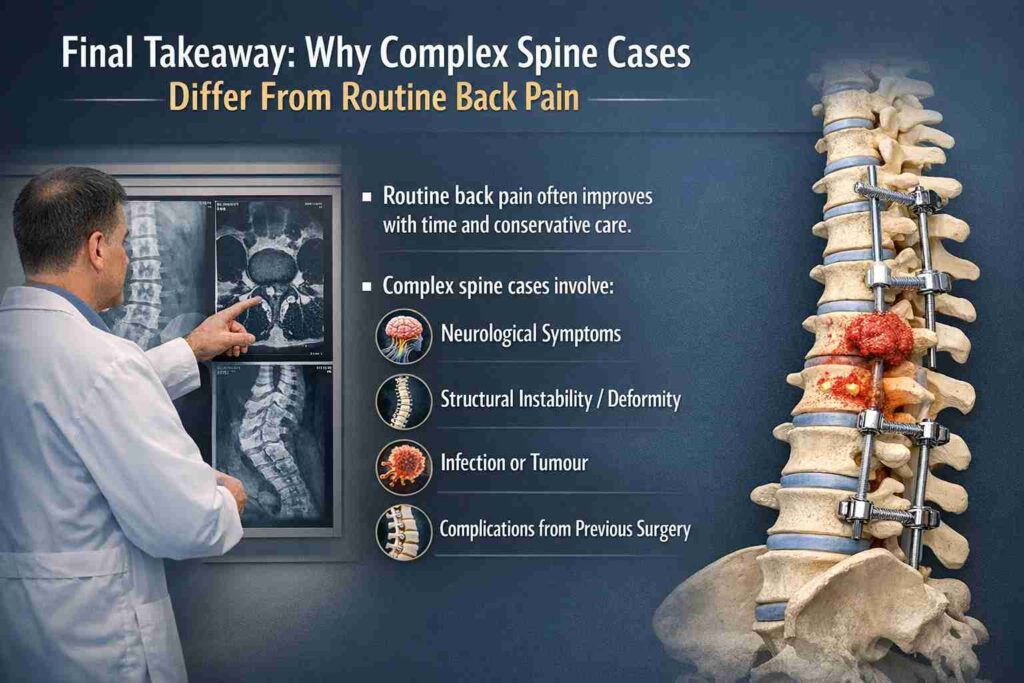
Routine mechanical back pain usually improves with posture changes, rest, and conservative care. Complex spine cases involve neurological symptoms, structural instability, deformity, infection, tumour, or complications of previous surgery, requiring specialised evaluation.
In clinical practice, doctors often begin by determining whether pain is mechanical or complex. The difference shapes everything from tests to treatment strategy.
What routine back pain usually looks like (strain, posture, early disc issues)
Most routine back pain is mechanical, often triggered by lifting, prolonged sitting, or poor posture. Typical signs include localised lower back pain, movement-related discomfort, relief with rest or position change, and no neurological symptoms.
Typical causes include:
| Cause | What Happens | Outcome |
| Muscle strain | Back muscles overstretched | Improves in days–weeks |
| Postural overload | Prolonged sitting, poor ergonomics | Improves with posture correction |
| Early disc irritation | Mild disc inflammation | Usually settles with conservative care |
Persistent symptoms may require evaluation by a spine specialist for severe back pain.
What “complex” usually means in spine care
In spine care, “complex” does not simply mean severe pain. They usually involve structural changes, neurological risk, or multi-level spinal involvement requiring specialist evaluation.
Doctors consider a case complex when it includes:
- Multiple spinal levels are affected
- Progressive nerve compression
- Structural deformity
- Infection or tumour affecting the spine
- Prior spinal surgery complications
These cases often require expert assessment by Dr Purnajyoti Banerjee, a spinal surgeon in London.
The 60-Second Self-Check: Red Flags That Make It “Not Routine”
Certain symptoms suggest the spine problem may involve nerves, infection, fracture, or tumour. These red flags require urgent evaluation rather than routine pain management. Recognising early warning signs helps prevent serious complications.
New or progressive weakness, numbness, or walking difficulty

Back pain accompanied by neurological symptoms – numbness, weakness in the legs, and back pain are emergency signs that require prompt medical assessment.
These signs may occur during sciatica (leg pain from the back), with severe nerve compression, or with other conditions.
Bladder/bowel issues, saddle numbness (urgent evaluation)
Loss of bladder or bowel control combined with back pain is rare but extremely serious.
This can indicate symptoms of CES (Cauda Equina Syndrome), a condition in which the spinal nerves controlling the pelvic organs are compressed. [Source].
Urgent symptoms include:
| Symptom | Why It Matters |
| Difficulty urinating | Nerve damage affecting bladder control |
| Loss of bowel control | Severe nerve compression |
| Saddle numbness | Numbness in the groin area |
These symptoms require emergency medical care.
Fever, unexplained weight loss, night/rest pain
Fever, unexplained weight loss, and persistent night or rest pain are warning signs that shouldn’t be ignored. When these symptoms occur without a clear cause, they may indicate an underlying condition and need prompt medical evaluation.
Major trauma/fall or known osteoporosis with sudden, severe pain
Sudden pain after a fall or minor trauma in people with fragile bones may signal a spinal fracture.
High-risk groups include:
- older adults
- people with osteoporosis
- those on long-term steroids
Early imaging helps detect fractures before complications develop.
The “Complex Spine” Bucket List: Conditions That Change Everything
Some spinal disorders go beyond routine back pain and fall into complex spine conditions. These problems often threaten spinal stability, affect nerves, or reflect underlying disease, requiring specialist spine care.
Spinal deformity
Abnormal curvature of the spine can lead to chronic pain, imbalance, and nerve compression. Severe cases may require scoliosis/kyphosis spine deformity surgery to restore alignment and stability.
Tumours (primary or metastatic)
Tumours (primary or metastatic) affecting the spine can arise from bone, nerve tissue, or spread from other cancers. Evaluation focuses on:
- tumour type
- spinal stability
- neurological risk
Management may involve oncology, surgery, and targeted therapies.
Infection (e.g., spondylodiscitis)
Spinal infections such as spondylodiscitis are serious bacterial infections affecting the intervertebral disc and nearby vertebrae, often causing severe localised back or neck pain and reduced mobility, with the potential to damage the disc and surrounding bone.
Symptoms may include:
- severe back pain
- fever
- fatigue
- progressive weakness
Early diagnosis prevents structural collapse.
Trauma and fractures (especially osteoporotic fractures)
Spinal trauma may occur after accidents or minor injuries in fragile bones. Doctors evaluate:
| Injury Type | Concern |
| Compression fracture | vertebral collapse |
| burst fracture | spinal canal narrowing |
| unstable fracture | neurological risk |
Instability / multi-level degeneration / severe stenosis with neurologic compromise
Advanced degenerative disease can narrow the spinal canal and compress nerves. This condition often appears as spinal stenosis symptoms, especially when walking becomes painful or limited.
Revision spine surgery (after a prior surgery or failed fusion)
Previous surgery changes anatomy and increases treatment complexity. Situations such as revision spine surgery / failed back surgery treatment require careful imaging and planning by a spinal surgeon experienced in complex revision procedures.
How Doctors Classify Severity: What Makes a Case “Complex” Clinically
Doctors classify spine cases based on neurological involvement, number of spinal levels affected, structural alignment, and prior surgery history. These factors determine risk and treatment approach.
Neurology: nerve root vs spinal cord involvement (and why that matters)
Nerve root compression causes: shooting leg pain, numbness and muscle weakness. Spinal cord compression can affect: balance, walking ability and coordination. These differences guide urgency and treatment decisions.
Number of levels involved and alignment problems
A single disc problem is usually simpler than a disease affecting multiple spinal levels. Multi-level degeneration increases surgical complexity and recovery planning.
Stability: Slip, fracture risk, deformity progression
Spinal stability determines whether the spine can safely support movement. Instability may result from: vertebral slippage, fracture and severe degeneration
Prior surgery history (scar tissue, hardware, altered anatomy)
Previous procedures create unique challenges. Those include
- scar tissue around nerves
- implanted hardware
- altered anatomy
These cases often require advanced surgical planning by a spinal surgeon.
Diagnosis Pathway: What Tests Are “Normal” and What’s for High-Risk Cases
Doctors use different diagnostic tools depending on symptom severity. Some patients only need basic imaging, while complex cases require advanced scans and laboratory testing.
When X-ray is enough vs when MRI becomes important
Basic imaging helps assess alignment and fractures.
| Test | What It Shows |
| X-ray | bone alignment and fractures |
| MRI | discs, nerves, soft tissue |
| CT scan | detailed bone structure |
MRI becomes essential when nerve compression or a tumour is suspected.
When blood tests are relevant (infection/inflammation suspicion)
Blood tests are used selectively when symptoms suggest systemic disease. Those conditions are namely
- infection markers
- inflammatory disease
- tumour indicators
Why “MRI findings” don’t automatically mean surgery
Seeing an abnormality on an MRI can sound alarming, but imaging results alone rarely decide treatment. Many people have disc bulges or degenerative changes on scans without experiencing any symptoms.
Doctors consider several factors before recommending surgery, including:
- Symptoms and how much pain affects daily life
- Neurological findings, such as numbness or weakness
- Functional limitations, including difficulty walking, standing, or performing routine activities
Treatment Pathway: Routine Back Pain Plan vs Complex Spine Plan
Routine back pain usually improves with conservative treatment. Complex cases require multidisciplinary care, advanced interventions, and, at times, carefully planned surgery.
Routine: activity modification, physio, meds, time (most improve)
Most patients recover with:
- physiotherapy
- exercise
- anti-inflammatory medication
- posture correction
Complex: multidisciplinary care + targeted interventions + sometimes surgery planning
Complex spine cases often involve a coordinated care team. Treatment options may include:
| Treatment Approach | Purpose |
| targeted injections | reduce nerve inflammation |
| specialised physiotherapy | restore mobility |
| surgical intervention | correct structural problems |
Why complex spine surgery has a higher complication risk than straightforward degenerative surgery
Complex procedures may involve:
- longer surgical time
- multiple spinal levels
- nerve decompression and stabilisation
Careful planning and experienced surgical expertise help minimise risks.
When to See Which Specialist
Knowing which specialist to consult can prevent delays in diagnosis and treatment for spine conditions.
Ortho spine vs neuro-spine vs pain specialist: who does what
Different specialists address different aspects of spine care.
| Specialist | Focus |
| Orthopaedic spine surgeon | bone and structural spine problems |
| Neurosurgeon | nerve and spinal cord conditions |
| Pain specialist | injections and non-surgical care |
People often wonder when to consult a back pain doctor, especially when symptoms persist beyond a few weeks.
When you should go straight to the emergency department
Emergency evaluation is required when symptoms include:
- sudden leg weakness
- bladder or bowel changes
- rapid neurological decline
These symptoms should never be ignored.
Early evaluation by Dr Purnajyoti Banerjee, a spinal surgeon in London, helps identify these conditions and guide appropriate treatment before permanent damage develops.
Book your consultation today at this email address: purnajyoti74@gmail.com.
People Also Ask
What to ask at the first appointment?
Ask about the diagnosis, treatment options, recovery expectations, warning symptoms, and whether my condition needs monitoring or urgent intervention.
How long is “too long” to wait before seeing a specialist?
If your back pain lasts longer than six weeks, worsens, or includes neurological symptoms, consult a specialist promptly.
Is leg pain always a sign of a slipped disc?
No. Leg pain can result from nerve irritation, spinal stenosis, muscle problems, or vascular issues, not just disc herniation.
Can bladder/bowel symptoms ever be “nothing serious”?
Rarely. Bladder or bowel changes with back pain may indicate serious nerve compression requiring urgent medical evaluation.